Each film coated tablet contains: Irbesartan 300 mg.
Pharmacology: Pharmacodynamics: Mechanism of action: Irbesartan is a potent, orally active, selective Angiotensin-II receptor (type AT1) antagonist. It is expected to block all actions of Angiotensin-II mediated by the AT1 receptor, regardless of the source or route of synthesis of Angiotensin-II. The selective antagonism of the Angiotensin-II (AT1) receptors result in increases in plasma renin levels and Angiotensin-II levels, and a decrease in plasma aldosterone concentration. Serum potassium levels are not significantly affected by Irbesartan alone at the recommended doses. Irbesartan does not inhibit ACE (kininase-II), an enzyme which generates Angiotensin-II and also degrades bradykinin into inactive metabolites. Irbesartan does not require metabolic activation for its activity.
Clinical efficacy: Hypertension: Irbesartan lowers blood pressure with minimal change in heart rate. The decrease in blood pressure is dose-related for once a day doses with a tendency towards plateau at doses above 300 mg. Doses of 150-300 mg once daily lower supine or seated blood pressures at trough (i.e. 24 hours after dosing) by an average of 8-13/5-8 mmHg (Systolic/diastolic) greater than those associated with placebo.
Peak reduction of blood pressure is achieved within 3-6 hours after administration and the blood pressure lowering effect is maintained for at least 24 hours. At 24 hours the reduction of blood pressure was 60-70% of the corresponding peak diastolic and systolic responses at the recommended doses. Once daily dosing with 150 mg produced through and mean 24 hours responses similar to twice daily dosing on the same total dose.
The blood pressure lowering effect of Irbesartan Tablets is evident within 1-2 weeks, with the maximal effect occurring by 4-6 weeks after start of therapy. The antihypertensive effects are maintained during long-term therapy. After withdrawal of therapy, blood pressure gradually returns toward baseline. Rebound hypertension has not been observed. The blood pressure lowering effects of Irbesartan and thiazide-type diuretics are additive. In patients not adequately controlled by Irbesartan alone, the addition of a low dose of hydrochlorothiazide (12.5 mg) to Irbesartan once daily results in a further placebo-adjusted blood pressure reduction at trough of 7-10/3-6 mmHg (systolic/diastolic). The efficacy of Irbesartan Tablets is not influenced by age or gender. As is the case with other medicinal products that affect the renin-angiotensin system, black hypertensive patients have notably less response to Irbesartan monotherapy. When Irbesartan is administered concomitantly with a low dose of hydrochlorothiazide (e.g., 12.5 mg daily), the antihypertensive response in black patients approaches that of white patients. There is no clinically important effect on serum uric acid or urinary uric acid secretion.
Paediatric population: Reduction of blood pressure with 0.5 mg/kg (low), 1.5 mg/kg (medium), and 4.5 mg/kg (high), target titrated doses of Irbesartan was evaluated in 318 hypertensive or at risk (diabetic, family history of hypertension) children and adolescents aged 6 to 16 years over a three-week period. At the end of the three weeks the mean reduction from baseline in the primary efficacy variable, trough seated systolic blood pressure (SeSBP) was 11.7 mmHg (Low dose), 9.3 mmHg (Medium dose), 13.2 mmHg (High dose). No significant difference was apparent between these doses. Adjusted mean change of trough seated diastolic blood pressure (SeDBP) was as follows: 3.8 mmHg (Low dose), 3.2 mmHg (Medium dose) and 5.6 mmHg (high dose). Over a subsequent two week period where patients were rerandomized to either active medicinal product or placebo, patients on placebo had increases of 2.4 and 2.0 mmHg in SeSBP and SeDBP compared to +0.1 and -0.3 mmHg changes respectively in those on all doses of Irbesartan.
Hypertension and type 2 diabetes with renal disease: The "Irbesartan Diabetic Nephropathy Trial (IDNT)" shows that Irbesartan decreases the progression of renal disease in patients with chronic renal insufficiency and overt proteinuria. IDNT was a double blind, controlled, morbidity and mortality trial comparing Irbesartan Tablets, Amlodipine and placebo. In 1,715 hypertensive patients with type 2 diabetes, proteinuria ≥900 mg/day and serum creatinine ranging from 1.0-3.0 mg/dL, the long-term effects (mean 2.6 years) of Irbesartan Tablets on the progression of renal disease and all cause mortality were examined. Patients were titrated from 75 mg to a maintenance dose of 300 mg Irbesartan Tablets, from 2.5 mg to 10 mg Amlodipine, or placebo as tolerated. Patients in all treatment groups typically received between 2 and 4 antihypertensive agents (e.g., diuretics, beta blockers, alpha blockers) to reach a predefined blood pressure goal of ≤135/85 mmHg or a 10 mmHg reduction in systolic pressure if, baseline was > 160mmHg. Sixty percent (60%) of patients in the placebo group reached this target blood pressure whereas this figure was 76% and 78 % in the Irbesartan and Amlodipine groups respectively. Irbesartan significantly reduced the relative risk in the primary combined end point of doubling serum creatinine, end-stage renal disease (ESRD) or all-cause mortality. Approximately 33% of patients in the Irbesartan group reached the primary renal composite end point compared to 39% and 41 % in the placebo and Amlodipine groups [(20% relative risk reduction versus placebo (p = 0.024) and 23% relative risk reduction compared to Amlodipine (p = 0.006)]. When the individual components of the primary end point were analyzed, no effect in all cause mortality was observed, while a positive trend in the reduction in ESRD and a significant reduction in doubling of serum creatinine were observed. Subgroups consisting of gender, race, age, duration of diabetes, baseline blood pressure, serum creatinine, and albumin excretion rate were assessed for treatment effect. In the female and black subgroups which represented 32% and 26% of the overall study population respectively, a renal benefit was not evident, although the confidence intervals do not exclude it. As for the secondary endpoint of fatal and non-fatal cardiovascular events, there was no difference among the three groups in the overall population, although an increased incidence of non-fatal MI was seen for women and a decreased incidence of non-fatal MI was seen in males in the Irbesartan group versus the placebo-based regimen. An increased incidence of non-fatal MI and stroke was seen in females in the Irbesartan-based regimen versus the Amlodipine-based regimen, while hospitalization due to heart failure was reduced in the overall population. However, no proper explanation for these findings in women has been identified. The study of the "Effects of Irbesartan on Microalbuminuria in Hypertensive patients with type 2 Diabetes Mellitus (IRMA 2)" shows that Irbesartan 300 mg delays progression to overt proteinuria in patients with Microalbuminuria, IRMA 2 was a placebo-controlled double blind morbidity study in 590 patients with type 2 diabetes, microalbuminuria (30-300mg/day) and normal renal function (Serum creatinine) ≤ 1.5 mg/dL in males and <1.1 mg/dL in females). The study examined the long-term effects (2 years) of Irbesartan Tablets on the progression to clinical (overt) proteinuria (urinary albumin excretion rate (UAER) > 300 mg/day, and an increase in UAER of at least 30% from base line).
The predefined blood pressure goal was ≤ 135/85 mmHg. Additional antihypertensive agents (excluding ACE inhibitors, Angiotensin II receptor antagonists and dihydropyridine calcium blockers) were added as needed to help achieve the blood pressure goal. While similar blood pressure was achieved in all treatment groups, fewer subjects in the Irbesartan 300 mg group (5.2%) than in the placebo (14.9%) or in the Irbesartan 150 mg group (9.7%) reached the end point of overt proteinuria, demonstrating a 70% relative risk reduction versus placebo (p= 0.0004) for the higher dose. An accompanying improvement in the glomerular filtration rate (GFR) was not observed during the first three months of treatment. The slowing in the progression to clinical proteinuria was evident as early as three months and continued over the 2-year period. Regression to normoalbuminuria (< 30 mg/day) was more frequent in the Irbesartan 300 mg Tablets group (34%) than in the placebo group (21 %).
Pharmacokinetics: After oral administration, Irbesartan is well absorbed: studies of absolute bioavailability gave values of approximately 60.80%. Concomitant food intake does not significantly influence the bioavailability of Irbesartan. Plasma protein binding is approximately 96%, with negligible binding to cellular blood components. The volume of distribution is 5393 liters. Following oral or intravenous administration of 14C Irbesartan, 80-85% of the circulating plasma radioactivity is attributable to unchanged Irbesartan.
Irbesartan is metabolized by the liver via glucuronide (approximately 6%). In vitro studies indicate that Irbesartan is primarily oxidised by the cytochrome P450 enzyme CYP2C9. Isoenzyme CYP3A4 has negligible effect. Irbesartan exhibits linear and dose proportional pharmacokinetics over the dose range of 10 to 600 mg. A less than proportional increase in oral absorption at doses beyond 600 mg (Twice the maximal recommended dose) was observed. The mechanism for this is unknown. Peak plasma concentrations are attained at 1.5-2 hours after oral administration. The total body and renal clearance are 157-176 and 3-3.5 mL/min, respectively. The terminal elimination half-life of Irbesartan is 11-15 hours. Steady state plasma concentrations are attained within 3 days after initiation of a once-daily dosing regimen. Limited accumulation of Irbesartan (< 20%) is observed in plasma upon repeated once-daily dosing. In a study, somewhat higher plasma concentrations of Irbesartan were observed in female hypertensive patients. However, there was no difference in the half-life and accumulation of Irbesartan. No dosage adjustment is necessary in female patients. Irbesartan AUC and Cmax values were also somewhat greater in elderly subjects (65 years) than those of young subjects (18-40 years). However, the terminal half-life was not significantly altered. No dosage adjustment is necessary in elderly patients. Irbesartan and its metabolites are eliminated by both biliary and renal pathways. After either oral or IV administration of 14C Irbesartan, about 20 % of the radioactivity is recovered in the urine, and the remainder in the faeces. Less than 2 % of the dose is excreted in the urine as unchanged Irbesartan.
Paediatric population: The pharmacokinetics of Irbesartan were evaluated in 23 hypertensive children after the administration of single and multiple daily doses of Irbesartan (2 mg/kg) up to a maximum daily dose of 150 mg for four weeks. Of those 23 children, 21 were evaluable for comparison of pharmacokinetics with adults (Twelve children over 12 years, nine children between 6 and 12 years). Results showed that Cmax, AUC and clearance rates were comparable to those observed in adult patients receiving 150 mg Irbesartan daily. A limited accumulation of Irbesartan (18%) in plasma was observed upon repeated once daily dosing.
Renal impairment: In patients with renal impairment or those undergoing haemodialysis, the pharmacokinetic parameters of Irbesartan are not significantly altered. Irbesartan is not removed by haemodialysis.
Hepatic impairment: In patients with mild to moderate cirrhosis, the pharmacokinetic parameters of Irbesartan are not significantly altered.
Studies have not been performed in patients with severe hepatic impairment.
Irbesartan is indicated in adults for the treatment of essential hypertension.
It is also indicated for the treatment of renal disease in adult patients with hypertension and type 2 diabetes mellitus as part of an antihypertensive medicinal product regimen.
Posology: The usual recommended initial and maintenance dose is 150 mg once daily, with or without food. Irbesartan Tablets at a dose of 150 mg once daily generally provides a better 24-hour blood pressure control than 75 mg. However, initiation of therapy with 75 mg could be considered, particularly in haemodialysed patients and in the elderly over 75 years. In patients insufficiently controlled with 150 mg once daily, the dose of Irbesartan Tablets can be increased to 300 mg, or other antihypertensive agents can be added. In particular, the addition of a diuretic such as hydrochlorothiazide has been shown to have an additive effect with Irbesartan Tablets.
In hypertensive type 2 diabetic patients, therapy should be initiated at 150 mg Irbesartan once daily and titrated up to 300 mg once daily as the preferred maintenance dose for treatment of renal disease. The demonstration of renal benefit of Irbesartan Tablets in hypertensive type 2 diabetic patients is based on studies where Irbesartan was used in addition to other anti-hypertensive agents, as needed, to reach target blood pressure.
Special Populations: Renal impairment: No dosage adjustment is necessary in patients with impaired renal function. A lower starting dose (75 mg) should be considered for patients undergoing haemodialysis.
Intravascular volume depletion: Volume and/or sodium depletion should be corrected prior to administration of Irbesartan Tablets.
Hepatic impairment: No dosage adjustment is necessary in patients with mild to moderate hepatic impairment. There is no clinical experience in patients with severe hepatic impairment.
Elderly patients: Although consideration should be given to initiating therapy with 75 mg in patients over 75 years of age, dosage adjustment is not usually necessary for the elderly.
Paediatric population: The safety and efficacy of Irbesartan in children aged 0 to 18 has not been established.
Route of Administration: Irbesartan Tablets should be taken orally with liquid, with or without food.
Experience in adults exposed to doses of up to 900 mg/day for 8 weeks revealed no toxicity. The most likely manifestations of overdose are expected to be hypotension and tachycardia; bradycardia might also occur from overdose. No specific information is available on the treatment of overdose with Irbesartan Tablets. The patient should be closely monitored, and the treatment should be symptomatic and supportive. Suggested measures include induction of emesis and/or gastric lavage. Activated charcoal may be useful in the treatment of overdose. Irbesartan is not removed by haemodialysis.
Hypersensitivity to the active substance or to any of the excipients. Second and third trimester of pregnancy.
Intravascular volume depletion: Symptomatic hypotension, especially after the first dose, may occur in patients who are volume and/or sodium depleted by vigorous diuretic therapy, dietary salt restriction, diarrhoea or vomiting. Such conditions should be corrected before the administration of Irbesartan Tablets.
Renovascular hypertension: There is an increased risk of severe hypotension and renal insufficiency when patients with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney are treated with medicinal products that affect the renin angiotensin-aldosterone system. While this is not documented with Irbesartan Tablets, a similar effect should be anticipated with Angiotensin-II receptor antagonists.
Renal impairment and kidney transplantation: When Irbesartan Tablets is used in patients with impaired renal function, a periodic monitoring of potassium levels and creatinine serum levels in case of poor kidney function is recommended. There is no experience regarding the administration of Irbesartan Tablets in patients with a recent kidney transplantation.
Hypertensive patients with type 2 diabetes and renal disease: The effects of Irbesartan both on renal and cardiovascular events were not uniform across all subgroups, in an analysis carried out in the study with patients with advanced renal disease. In particular, they appeared less favorable in women and nonwhite subjects.
Hyperkalaemia: As with other medicinal products that affect the renin-angiotensin-aldosterone system, hyperkalaemia may occur during the treatment with Irbesartan Tablets, especially in the presence of renal impairment, overt proteinuria due to diabetic renal disease, and/or heart failure. Close monitoring of serum potassium in patients at risk is recommended.
Lithium: The combination of lithium and Irbesartan is not recommended.
Aortic and mitral valve stenosis, obstructive hypertrophic cardiomyopathy: As with other vasodilators, special caution is indicated in patients suffering from aortic or mitral stenosis, or obstructive hypertrophic cardiomyopathy.
Primary aldosteronism: Patients with primary aldosteronism generally will not respond to antihypertensive drugs acting through inhibition of the renin-angiotensin system. Therefore, the use of Irbesartan Tablets is not recommended.
General: In patients whose vascular tone and renal function depend predominantly on the activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive heart failure or underlying renal disease, including renal artery stenosis), treatment with Angiotensin converting enzyme inhibitors or Angiotensin-II receptor antagonists that affect this system has been associated with acute hypotension, azotaemia, oliguria, or rarely acute renal failure. As with any antihypertensive agent, excessive blood pressure decrease in patients with ischemic cardiopathy or ischemic cardiovascular disease could result in a myocardial infarction or stroke. As observed for Angiotensin converting enzyme inhibitors, Irbesartan and the other Angiotensin antagonists are apparently less effective in lowering blood pressure in black people than in non-blacks, possibly because of higher prevalence of low renin states in the black hypertensive population.
Lactose: This medicinal product contains lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Use in Pregnancy: Angiotensin II Receptor Antagonists (AIIRAs) should not be initiated during pregnancy. Unless continued AIIRA therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with AIIRAs should be stopped immediately, and, if appropriate, alternative therapy should be started.
Use in children: Irbesartan has been studied in paediatric populations aged 6 to 16 years old but the current data are insufficient to support an extension of the use in children under 16 years of age until further data become available.
In placebo-controlled trials in patients with hypertension, the overall incidence of adverse events did not differ between the Irbesartan (56.2%) and the placebo groups (56.5%). Discontinuation due to any clinical or laboratory adverse event was less frequent for Irbesartan treated patients (3.3%) than for placebo treated patients (4.5%). The incidence of adverse events was not related to dose (in the recommended dose range), gender, age, race, or duration of treatment. In diabetic hypertensive patients with micro albuminuria and normal renal function, orthostatic dizziness and orthostatic hypotension were reported in 0.5% of the patients (i.e., uncommon) but in excess of placebo.
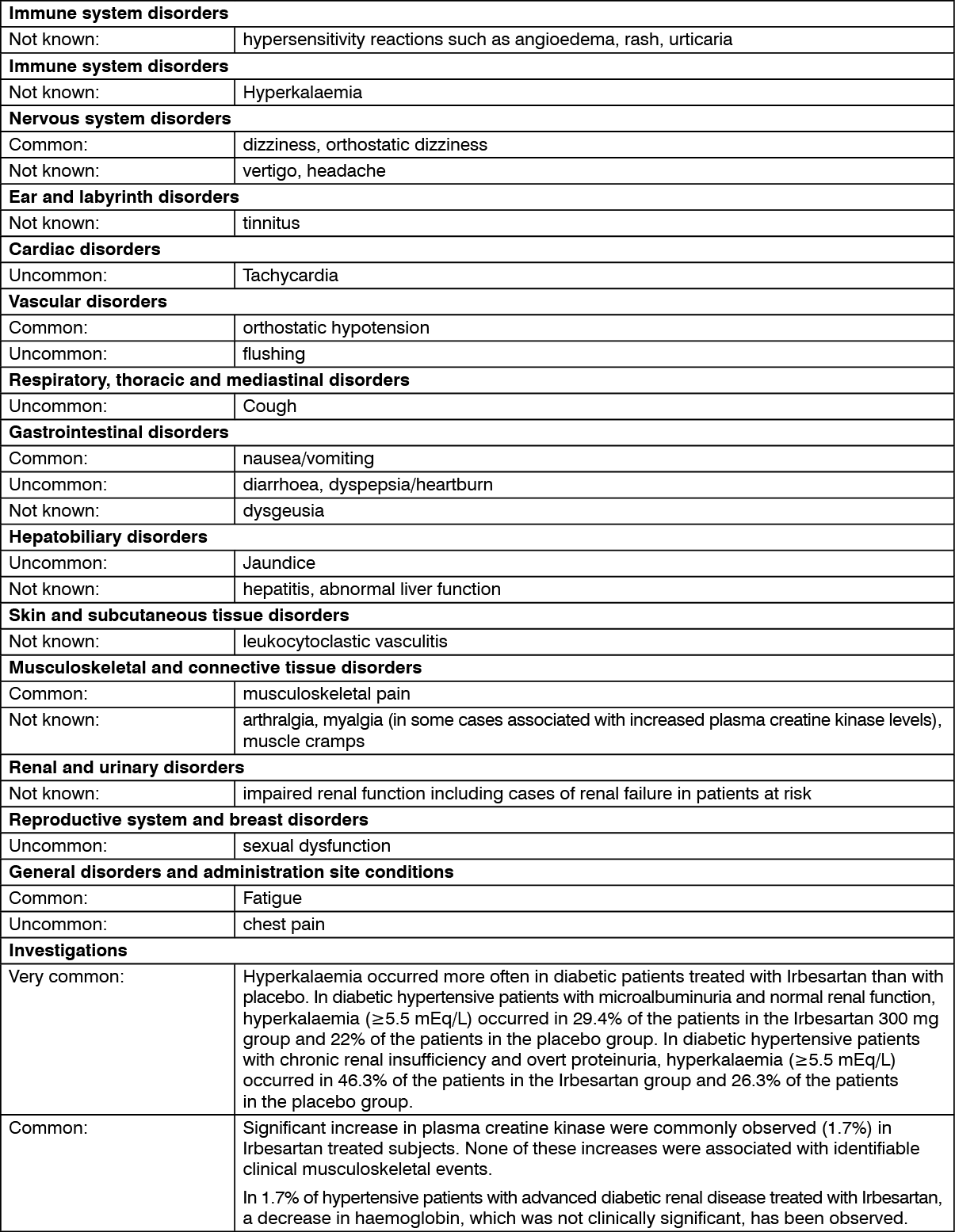
The following table presents the adverse drug reactions that were reported in placebo-controlled trials in which 1,965 hypertensive patients received Irbesartan. Terms marked with a star (*) refer to the adverse reactions that were additionally reported in > 2% of diabetic hypertensive patients with chronic renal insufficiency and overt proteinuria and in excess of placebo.
The frequency of adverse reactions listed as follows is defined using the following convention: Very common (≥ 1/10); common (≥ 1/100, < 1/10); Uncommon (≥ 1/1000, < 1/100); Rare (≥ 1/10,000, < 1/1,000); Very rare (< 1/10,000). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Adverse reactions additionally reported from post marketing experience are also listed. These adverse reactions are derived from spontaneous reports. (See table.)
 Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Paediatric population: In a randomized trial of 318 hypertensive children and adolescents aged 6 to 16 years, the following adverse reactions occurred in the 3-week double-blind phase: headache (7.9%); hypotension (2.2%); dizziness (1.9%); cough (0.9%). In the 26-week open-label period of this trial the most frequent laboratory abnormalities observed were creatinine increases (6.5%) and elevated CK values in 2% of child recipients.
Diuretics and other antihypertensive agents: Other antihypertensive agents may increase the hypotensive effects of Irbesartan; however, Irbesartan has been safely administered with other antihypertensive agents, such as betablockers, long-acting calcium channel blockers, and thiazide diuretics. Prior treatment with high dose diuretics may result in volume depletion and a risk of hypotension when initiating therapy with Irbesartan Tablets.
Potassium supplements and potassium sparing diuretics: Based on experience with the use of other medicinal products that affect the renin-angiotensin system, concomitant use of potassium-sparing diuretics, potassium supplements, salt substitutes containing potassium or other medicinal products that may increase serum potassium levels (e.g. heparin) may lead to increases in serum potassium and is, therefore, not recommended.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with Angiotensin converting enzyme inhibitors. Similar effects have been very rarely reported with Irbesartan so far. Therefore, this combination is not recommended. If the combination proves necessary, careful monitoring of serum lithium levels is recommended.
Non-steroidal anti-inflammatory drugs: When Angiotensin II antagonists are administered simultaneously with non-steroidal anti-inflammatory drugs (i.e., Selective COX-2 inhibitors, acetylsalicylic acid >3g/day and nonselective NSAIDs), attenuation of the antihypertensive effect may occur. As with ACE inhibitors, concomitant use of Angiotensin II antagonists and NSAIDs may lead to an increased risk of worsening of renal function, including possible acute renal failure, and an increase in serum potassium, especially in patients with poor pre-existing renal function. The combination should be administered with caution, especially in the elderly. Patients should be adequately hydrated and consideration should be given to monitoring renal function after initiation of concomitant therapy, and periodically thereafter.
Additional information on Irbesartan interactions: In clinical studies, the pharmacokinetics of Irbesartan is not affected by hydrochlorothiazide.
Irbesartan is mainly metabolised by CYP2C9 and to a lesser extent by glucuronidation. No significant pharmacokinetic or pharmacodynamic interactions were observed when Irbesartan was co-administered with warfarin, a medicinal product metabolised by CYP2C9. The effects of CYP2C9 inducers such as rifampicin on the pharmacokinetics of Irbesartan have not been evaluated. The pharmacokinetics of digoxin was not altered by co-administration of Irbesartan.
Store at temperatures not exceeding 30°C.
C09CA04 - irbesartan ; Belongs to the class of angiotensin II receptor blockers (ARBs). Used in the treatment of cardiovascular disease.
Virbez 300 FC tab 300 mg
28's (P686/box, P24.5/film-coated tab)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out